The challenge of localization in the SDGs: CartONG’s experience in the DRC
CartONG concluded in December 2018 a project to build a “data collaborative” in DRC to improve the measure of SDGs around health thanks to crowd-sourcing and in particular OpenStreetMap. But as usual in DRC, things turned out to be a little more complex than anticipated… Here is the story of this project!
This project funded by the Global Partnership for Sustainable Development Data (GPSDD, under the UN Foundation) was led by 510/Netherland Red Cross and targeted to develop the data collaborative approach in two countries, in Malawi (510) on WASH data, and in DRC (CartONG) on health data. We implemented in partnership with the OpenStreetMap DRC team.

Our goal was rather simple: to improve the measurement, and more specifically the localization, of SDG 3.8 “Achieve universal health coverage, including financial risk protection, access to quality essential health-care services and access to safe, effective, quality and affordable essential medicines and vaccines for all” and more precisely its first target indicator on the coverage of essential health services.
After reviewing the current reporting on SDGs available, we identified a gap in the measurement of this indicator (lack of baseline data and methodology to survey it accurately). Based on the localization plan for the province of Tanganyika (the national one not being available yet), we focused on the 2 indicators for which our participatory methodology could be the most effective, i.e. the percentage of population covered by basic and advanced health services (health centers and hospitals).
Our strategy to improve the measure of these indicators was the following: first, to assemble the existing data with all local stakeholders and assess its quality. Then, improve it on at least one pilot area with a field mission. And finally, build analysis tools to make use of the collected and curated data for the measure of SDGs.
A data collaborative to share health data in DRC
As presented in our previous news, the project kicked off in January 2018 with an inception workshop in Kinshasa co-organized with the DRC Red Cross. The workshop allowed us to assess the current “landscape” of data on health and we identified a strong need to first improve the baseline data (location of health sites, as well as delimitation of health areas which are the basic surveying unit). In the following months, we implemented – in Kinshasa and also remotely – the actions defined with the various stakeholders during the workshop, including:
- Supporting the local stakeholders in sharing health data, by relaunching and facilitating the Référentiel Géographique Commun’s health group and communicating regularly to other actors, in particular the IM working group and of course the Ministry of Health (MoH, Ministère de la Santé Publique), and also running OSM introduction workshops with several actors.
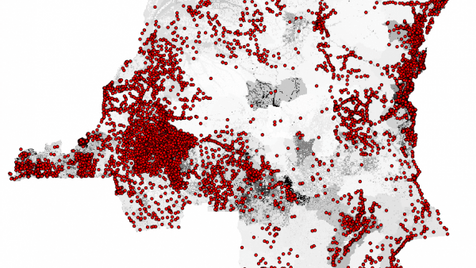
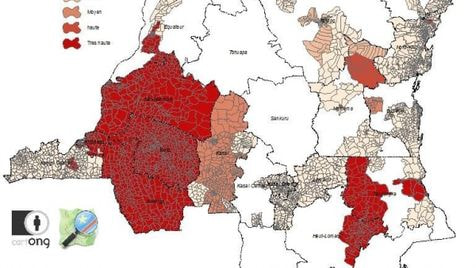
- A vast effort to gather all existing data on health areas and health sites in DRC that various organizations (NGOs, universities, UN agencies, etc., coordinating with the project GRID3) had collected over the years: more than 12,300 health sites (7,000 geo-located) and 5,300 health areas (on an estimated total of around 9,000), unequally distributing over the country. This also included the definition of a quality referential that has since then allowed us to assess the quality of the data collated (cf. maps below). The collected and assessed data has been shared in beta via the RGC and is currently pending official approval, while the RGC team still continues updating it.
- Simultaneously to the data curation process, we built and updated the RGC data model matching the attributes in OpenStreetMap (building on the work already done by Healthsites.io), as well as finalizing a methodology to delineate precisely health areas with field MoH staffs.
Two field pilots to collect data and test our methodologies
Following this preparation work, we used this data model in the 2 field missions conducted in partnership, first with the Intercluster in May, and second with the Ministry of Health in September, in order to test the possibility of quality data collection on both health sites and health areas boundaries. The missions were co-implemented with OSM DRC, one of the goal being to directly collect the health sites data in OSM. The field pilots confirmed several challenges we were expecting to encounter:
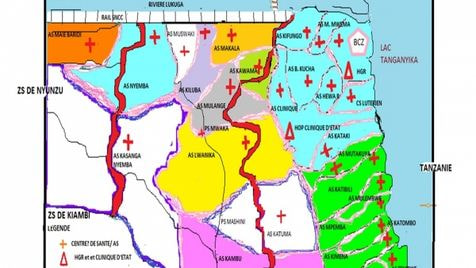
- The quality of the existing health areas boundaries, currently used by many actors, is very limited (when they even exist), as shown on the map below (in orange before/in red after redrawing the delineation based on local knowledge), also compared with the sketch which was the only map available to field workers. This weakens the whole data collection on health indicators in the country, including SDGs, since the DHIS2 and other statistics systems are aggregating data based on an incorrect picture of the field through these distorted health areas.

- The methodology used for health areas delineation, based on direct feedback from the local “infirmiers titulaires” (head nurses from a health area) gave accurate results for a reduced cost and time invested.

- The data model for health sites also proved adapted, with 50 health sites enumerated and directly uploaded in OpenStreetMap and usable for analysis (cf. below). An introduction to the mobile data collection method used (KoBo Toolbox) was also presented to local MoH workers.
- There are important gaps in data collection, not only for geographic information but more generally speaking for all health data collected in the field, demonstrated by the numerous heavy piles of unpacked paper forms visible in many local offices.
- Providing local teams with tools or equipment is not enough if no long-term back-up is provided to them both in terms of technical help but also financial support. No quality data collection can be expected from field offices as long as they have to struggle to obtain basic things (cash for periodic internet access, salaries, basic equipment, etc.).
- The collaborative work has proved to work also in the field, not only by the success of missions involving multiple actors (CartONG/OSM DRC, CERF, IOM, MoH) but also with the local MoH teams that have proven consistent interest on the approach and its deliverables.
Building analysis tools and training actors on them
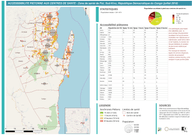
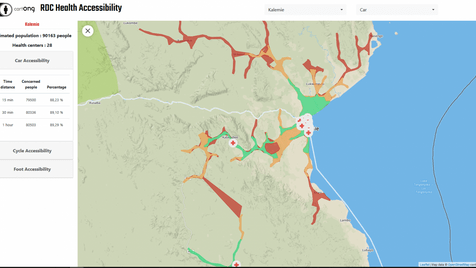
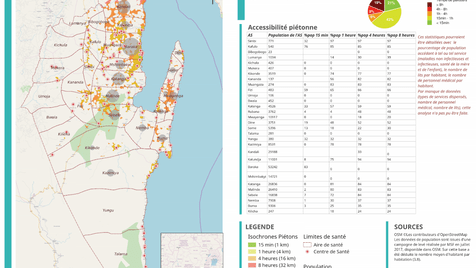
The data collected during the mission then allowed to build several analysis products including paper maps analyzing the accessibility of health centers for the population as well as a prototype dashboard allowing a dynamic and upgradeable analysis based on OSM data thanks to the OpenRouteService, developed by the University of Heidelberg.
A second workshop (coupled with several bilateral meetings since many actors couldn’t join us due to the ongoing Ebola outbreak) was organized in July which allowed to present the advances of the previous months, get feedback from stakeholders on the first mission and define the strategy for the finalization of the project.
A general look back
This project, conducted simultaneously in two very different countries, has allowed CartONG and 510 to highlight the following lessons learned:
- the importance of open standards to increase collaboration and interoperability;
- the need for participatory approaches in the development of technology and data tools;
- the importance of broad multi-stakeholder engagements and convergence in use of supporting platforms instead of divergence;
- the need for localizing the SDGs to give them contextual and cultural relevance;
- the importance of developing technology solutions that enhance the freedom and capabilities of the collaborating communities while remaining accessible (reduced cost and complexity);
- the need to find operational uses of the data & methodologies shared for stakeholders, in order to get buy-in in the data sharing process and ensure sustainable update by them (this also entails finding shared methods for humanitarian and development organizations whenever possible);
- the importance of quality of data collection/collation methods including at field level to avoid the “garbage in/garbage out” effect.
We also encourage you to read the paper “Characterizing Data Ecosystems to Support Official Statistics with Open Mapping Data for Reporting on Sustainable Development Goals” published by Marc Van den Homberg & Iryna Susha (from 510) in the Special Issue “Geo-Information and the Sustainable Development Goals (SDGs)” of the ISPRS International Journal of Geo-Information, which develops the scientific approach of the overall project.
The effort made in 2018 will now be continued by the RGC community but also thanks to two projects which bear similar objectives, GRID3 (conducted by CIESIN) and CP3 (IFRC & DRC Red Cross). We are therefore confident that our time-bound contribution will help all actors improve the services provided to the Congolese people by giving them access to better data. Big thanks also to the OpenStreetMap DRC community and Claire and Christian in particular for their support!
CartONG is very interesting in continuing working improving the health data in DRC, as well as exploring the potential of OpenStreetMap & open data for SDGs measuring – please get in touch if you would like to collaborate with us on the topic!
